In debates about what the NHS should do to improve its performance it is common to see benchmarks of staffing or bed numbers versus comparable health systems. The argument is that the system needs more doctors/nurses/beds. This is not the biggest problem. The NHS has suffered far more from a failure to invest in capital, innovation or management.
Charts like the one below dominate the debate about NHS funding:
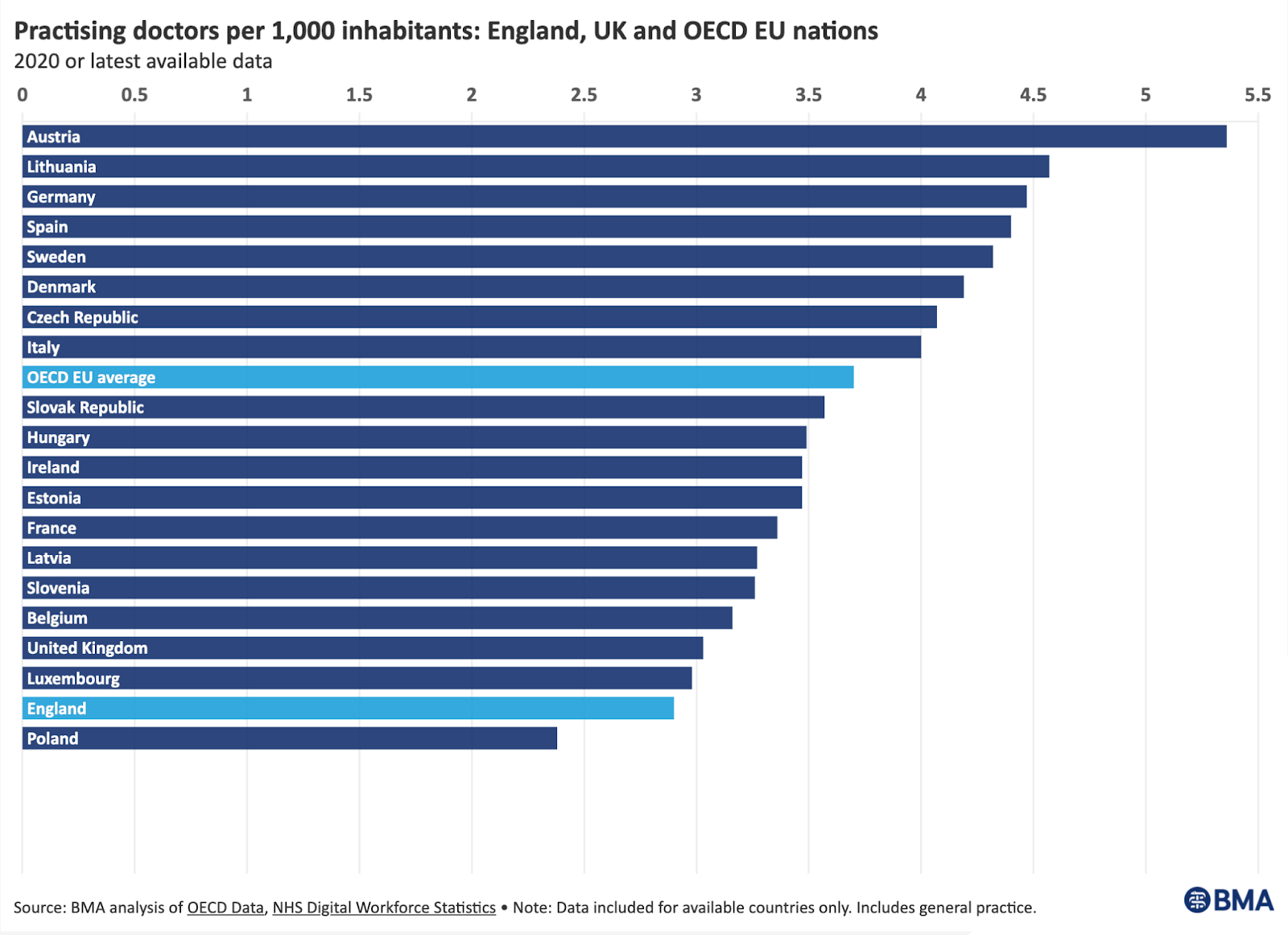
The message is simple: the NHS is underfunded and needs to have more doctors (or nurses or more money, depending on which lobbyist is producing the charts).
The implication is that the very obvious performance problems of the system would be solved if only we matched the same level of doctors/nurses/funding as the peer group of other health systems.
There is some debate on the strict comparability of these metrics and that is rarely mentioned by the lobbyists. In fact I once saw Nigel Edwards heckled for pointing out that a major revision on OECD metrics of overall spend on the NHS and comparable systems made the NHS look middling rather than an outlier on the low side. People really want the explanation for poor NHS performance to be simple and, preferably, a conspiracy they can blame on the Conservatives. It is frequent to see phrases like "Tory staffing cuts". And that is the end of the debate for many.
But, even though the overall NHS budget saw unusually low growth in the decade after 2010, front line staffing increased significantly. The "tory cuts" in staffing led to ~30% more doctors and 15% more nurses:

I don't want to argue that the government is not to blame. I do want to argue that we are looking in completely the wrong place about where policy has been wrong.
There are far, far bigger problems than not having enough front line staff. And the real problems that front line staff experience are often consequences of those other failures. Worse, those other failures get almost no attention and the topics that do get attention distort the debate so much that the biggest and most important failures get essentially no critical attention.
Before I get to the other issues that I argue matter more than staffing, it is worth a quick review of why the staffing benchmarks are not that relevant to NHS performance.
One reason is a lack of strict comparability with the other countries in how they use staff. But a more interesting one is that the implied policy when it looks like the NHS is behind ("fix the staffing, fix the problem") very clearly doesn't work in specific cases. An example is A&E staffing. It has been repeatedly claimed in the last decade that the decline in A&E performance is a consequence of a lack of A&E staff. But the number of A&E doctors rose faster than demand every year since 2010 and the number now is >30% higher than it was in 2010. The number of A&E specialists grew faster than any other for most of the last decade. But performance has declined monotonically over that period.
In this case it is easy to see why staffing was never the problem. Patients suffer long waits in A&E not because there are not enough A&E staff to treat them but because there are no free beds to move the patients to. This was known in the early 2000s when the 4hr target was set and has repeatedly been shown in detailed analysis of the causes of waits in the last decade (see, for example, this from Monitor). To put it simply, more A&E doctors can't magic up more free beds. They mostly can't even influence the number of free beds. So adding more staff doesn't fix the underlying problem. (I should add that the longer the A&E queue, the more staff are needed to handle it. So the apparent staff shortages are actually a symptom of a different problem elsewhere in the hospital, not the cause of the problem. Adding more doesn't fix the problem.)
So what other errors has the NHS made?
The NHS benchmarks that really matter
Let me tell you the answer before working through the details and arguments.
The NHS might be slightly short of front line staff but it is catastrophically short of support staff like managers and has a long standing lack of investment in innovation and capital spending. If benchmarks versus comparable health systems are any guide, the NHS is a spectacular outlier in investment and management.
The NHS is very undermanaged
When the Lansley Reforms were in draft form and proposed severe cuts in management numbers there were several analyses that criticized this goal. The King's Fund concluded as part of its commission on leadership and management that:
"If anything, our analysis seems to suggest that the NHS, particularly given the complexity of health care, is under–rather than over–managed."
And this was before the drastic cuts in the Lansley reforms were implemented (see the staffing chart above for their immediate impact). A more recent analysis (in a report by Ian Kirkpatrick and Becky Malby for the NHS Confederation) said:
"...it is hard to argue that the NHS is ‘overmanaged’. At approximately 2 per cent, managers are a very small proportion of the NHS workforce. By comparison, ‘managers, directors and senior officials’ in the UK as a whole make up 9.5 percent of the workforce."
And, in another report in the series they argued this:
"We found that even a small increase in the proportion of managers employed (from 2 to 3 per cent of the workforce in an average acute trust) had a marked impact.
Up to a certain point, larger management functions in trusts were associated with higher patient satisfaction scores, a 5 per cent rise in hospital efficiency and a 15 per cent reduction in infection rates. Further tests revealed that it was primarily higher levels of managers employed that drove these improvements and not the other way round."
Both NHS management numbers and total administration costs are far below international norms and have fallen sharply since 2010. Given the clear evidence from Kirkpatrick's work that more managers make hospitals function more effectively, cutting management looks like a bad error. Adding more managers has a lot of leverage over the performance of all the other staff but the NHS has chosen to cut their numbers instead.
Both manager numbers and total administrative costs are far more out of line with international norms than the number of doctors, nurses or beds. Although good comparable metrics are hard to find, the IFS claimed this in 2018:
The OECD has compiled data on administrative costs of different health care systems at the ‘macro’ level – which captures the amount spent on planning, funding and monitoring care, but not administrative costs within individual hospitals.
They found that the NHS spends relatively little on overseeing and planning care, relative to other comparable systems. In 2014, the UK, Portugal and Ireland all devoted 1.5% or less of their government or compulsory health care expenditure to administration. This compares with an average of 3.1%, with 4.1% in France, and 7.9% in the United States.
Investment in innovation and capital is grotesquely low
Another area where the NHS is an outlier is spending on capital and innovation. In fact it is an extreme outlier.
This is somewhat ironic given Rishi Sunak's recent spring statement where he diagnosed a major problem for the UK economic productivity as being largely caused by a lack of investment in innovation and capital. As he argued:
"Over the last fifty years, innovation drove around half the UK’s productivity growth.
…our lower rate of innovation explains almost all our productivity gap with the United States.
Right now, we know that the amount businesses spend on R&D as a percentage of GDP is less than half the OECD average.
…
Weak private sector investment is a longstanding cause of our productivity gap internationally:
Capital investment by UK businesses is considerably lower than the OECD average of 14%.
And it accounts for fully half our productivity gap with France and Germany."
The NHS is the largest part of the UK economy controlled by the government. So exactly how has the government sought to control its spending on the key factors that determine productivity in the rest of the economy?
It won't surprise you to know that it is the opposite of the Sunak recipe for productivity in the private sector.
The Health Foundation did a (little read) briefing on this in 2019. It starts by pointing out the obvious:
"Capital spending is a critical input in health care, with new technology able to transform services and improve workforce productivity.
The DHSC has proposed a more technology–and data–driven NHS. New technology and IT could improve patient services and increase productivity, but both currently make up a small proportion of capital spending."
So the DHSC has an ambition to exploit technology and IT (which needs investment). But the Health Foundation analysis of 20 years of NHS capital spending compared to peer health systems looks like this:
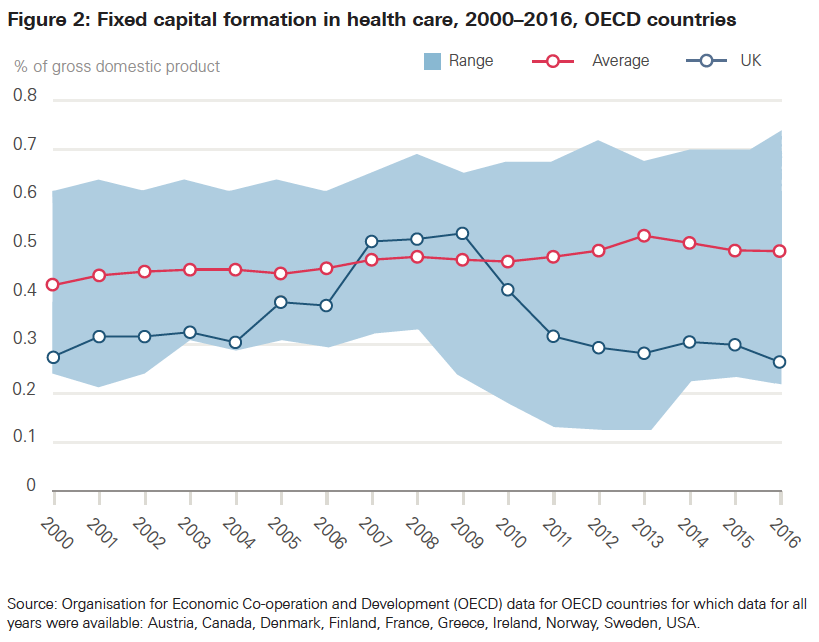
Only during the late Blair/Brown years did NHS capital spending come close to international norms and it is often the lowest or next to lowest in the whole dataset. The Health Foundation argue:
"For the UK to move up to the average for OECD countries, capital spending would have to almost double as a share of total health spending"
The National Audit Office also reviewed capital spending in the NHS in 2020 and some of their analysis tells an even more sorry tale.
They start by pointing out part of the current situation with buildings and other capital assets:
Parts of the NHS estate do not meet the demands of a modern health service. NHS hospitals include Victorian-era buildings, and 14% of the NHS estate predates the formation of the NHS (1948).
…
The growth in backlog maintenance indicates that there is an increased risk of harm to patients … the backlog of maintenance work to restore buildings to an appropriate standard was around £6.5 billion … High-risk backlog maintenance currently stands at £1.1 billion, and grew by 139% between 2014-15 and 2018-19, indicating an increased risk of harm to patients.
It isn't just the lack of modern IT and diagnostic equipment that holds back the NHS. It needs more modern buildings to do a good job but frequently doesn't have them. Worse, in some cases, maintenance problems in the existing buildings are so bad they risk immediate harm to patients.
Given this already disturbing background it might be a surprise when they point out that in many years of the last decade the already inadequate capital allocation to the NHS was underspent:
"Between 2010-11 and 2012-13, there was an average underspend of £677 million (12%) against the capital spending limit. In 2017-18, £360 million (6%) was unspent."
And their story gets worse:
"Since 2014-15 the Department has transferred £4.3 billion from capital to revenue spending"
So not only does the NHS start with an inadequate budget, which it underspends, it is then encouraged to pilfer the capital budget to cover operating costs. The reason this has been encouraged is because it is a convenient short term way to cover up operating deficits. These are embarrassing. And, obviously, avoiding embarrassment is more important than the roof of an operating theater falling in. Better still, while operating deficits are visible every year, most of the catastrophes from the maintenance backlog will appear slowly over a decade.
It might seem strange that the inadequate capital budget should ever be underspent. But the NAO explain that too by pointing out that the paperwork and bureaucracy of applying for capital is so baroque that many hospitals can't even get their cases for urgent maintenance past the system. And, even if they do, they might lose the allocation if they can't spend the money in-year as next year's allocation may be arbitrarily different. Short term changes to the budget every year make long term planning of capital spending impossible.
The buildings are inadequate for modern healthcare activities. There is a huge and rising backlog of maintenance to keep the show on the road that is limiting the capacity of the system to do more work. The system frequently steals from capital to employ more staff who will have to work in an environment where their work will be harder and less productive. The NHS is close to bottom on international rankings of the amount of high-tech equipment it needs to do the diagnostics necessary to tackle long elective queues. And there is little budget for investing in better IT to enable front line staff to work faster and more productively without the burden of coping with decade-old kit.
It is lucky that investing in capital or innovation doesn't matter for productivity. Oh, wait, that's exactly what the chancellor blamed for low productivity.
As an ironic coda to this section the following story appeared in the HSJ the day after his spring statement:
"Tech spend under pressure as NHSE told to ‘cut core funding’"
It hasn't taken long for the promises in the last spending review to invest more capital in the NHS to hit the buffers of old Treasury munchkin habits.
The government's goals for an improved, more productive NHS are directly undermined by its choices about how to allocate resources.
There are several important messages here.
Problem 1: the government itself has correctly argued that spending on capital and innovation are vital for driving up productivity. So much so that they are increasing the incentives to encourage more such spending in the private sector. But, when they control the budget, they do exactly the opposite. And, at the same time, continue to demand even higher productivity gains from the NHS. Whipping a dead horse doesn't cover it. It is more like whipping the reliquary containing the ashes of the horse cremated a decade ago after being euthanized for breaking a leg.
The second huge problem here is the lack of attention this analysis has had among commentators and the media. The news is full of stories about how the NHS is struggling because it has 10 or 20% fewer doctors than comparable systems. Lobbyists for nurses and doctors demand higher levels of staffing to fix the overwork, the current catastrophic waiting lists and A&E delays. But there is little mention of the fact that the NHS has perhaps half the capital employed per worker than almost any other health system. The NHS is a far more extreme outlier on this than it is on staffing. And the day to day work the front line staff have to do is much harder and less productive as a result.
The third problem is management. NHS management does make the news more often than capital spending, but almost always to disparage it. Stories often argue that we could cut management even further to put more resources to the front line. These stories usually fail to note that NHS management has already been sharply cut by the Lansley reforms and is currently another major outlier in comparisons between the NHS and other systems (I made the case about managers and their importance in the NHS here). Nor do they mention that very clear work shows that more managers make productivity and medical quality better.
In short, there is a fundamental mismatch between the government goal for a more productive NHS and the way it provides the tools to the NHS to achieve that productivity. The government and NHSE are like an army who recognises the need for bullets but forgot to allocate a budget for the guns required to fire them.
The perpetual failure to invest enough in capital, innovation or management is a far bigger problem for the NHS than any shortage of staff. It is about time the commentariat, the media and the government realized this. We won't fix the NHS until they do.
Learned a lot reading this. Thanks. The NAO reports seem to be pretty well universally great. They also appear not to be read much in Government, sadly. You note that it's really just BaU for the Treasury Munchkins, so it seems likely that this is a problem across all aspects of Government, not just the NHS - just most visible in the NHS. Until the Treasury stops impeding capital spending in general, the situation is unlikely to improve in the NHS.
ReplyDelete