The NHS is a microcosm of the British economy

Mistakes in how the government has managed the NHS parallel the mistakes in managing the economy. Trying to hold down the government budget is constantly approached by making easy choices rather than the right choices. The same is true in the NHS where the capital budget is raided to cover operating deficits. Both are recipes for long term decline.
All governments would like to see a higher growth rate in the economy. The current one wants to increase incentives with tax cuts but need to pay for those giveaways with spending cuts. But, faced with those spending challenges, they often take the easy road to keep the budget in some sort of balance by cutting the very capital projects that might improve growth in the long term.
The parallel with the NHS is interesting. Growth in spending seems relentless. That growth can be constrained only by improving productivity. But the choices made to keep the budget under some semblance of control hurt productivity, making tomorrow's problems worse. In this way the NHS is like a microcosm of the whole economy, at least in the ways both have been managed in the last decade or two.
The economy
The link is explained by the factors known to affect productivity in the economy and the NHS.
As Sunak explained in his spring statement while he was still chancellor (my highlighting)
"Over the last fifty years, innovation drove around half the UK’s productivity growth.
…our lower rate of innovation explains almost all our productivity gap with the United States.
Right now, we know that the amount businesses spend on R&D as a percentage of GDP is less than half the OECD average.
…
Weak private sector investment is a longstanding cause of our productivity gap internationally:
Capital investment by UK businesses is considerably lower than the OECD average of 14%.
And it accounts for fully half our productivity gap with France and Germany."
His analysis is mainstream economics. But it is worth asking what governments have actually done about either innovation or capital spending over the last decade or two because the same factors matter not just in the private sector but in the parts of the economy controlled by the government.
This chart on total government spending appeared recently in the FT:

The point is that, when faced with alternative ways to control total government spending, Osbourne chose the easy path of cutting capital spending, not current spending. And that spending on national infrastructure is the sort of thing that leads to long term improvement in productivity (and there is a direct influence on the economics of private capital spending because the future returns on that will be higher if the national infrastructure is better).
But, politically, capital is easier to cut. Who notices the long term impact of projects that might not finish for years and might only show big benefits in decades? Everyone can see this year's budget deficit. The temptation is to take the easy option even though it is the worse option for productivity and growth in the long term. Yes, all politicians, if asked, would claim they want higher productivity and growth: but they are very reluctant to face worse headlines tomorrow about the budget deficit.
Given that UK productivity growth tanked during the Osbourne austerity period, you might think this lesson had been learned. But that is not what the mood music emerging from Whitehall suggests where, in response to the catastrophic reception of the Kwarteng mini-budget, departments are being asked to make sharp cuts with capital spending at the top of the list.
The NHS
How governments have managed the NHS is a microcosm of this same problem. And it has been catastrophic for the long term health of the system.
If tomorrow's NHS is to be less of a financial burden on future governments, it needs to be much more productive (however that is defined: quality and throughput both matter in healthcare). The same factors–innovation and capital–have big influences on future NHS productivity. But how has the budget been allocated in the last decade or two?
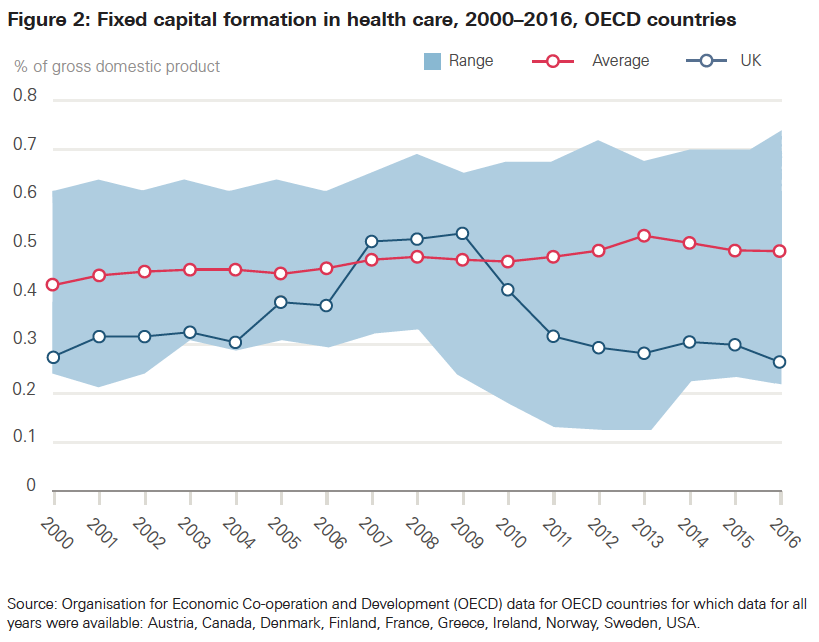
We can compare the NHS to other health systems in how it allocates money to the things that should matter to future productivity. The easiest to measure is capital spending. And, mirroring the problem with spending in the economy as a whole, the big picture looks to be a catastrophe of poor short term choices (for a more detailed analysis see my longer rant here). In an analysis in 2019, the Health Foundation produced this chart:
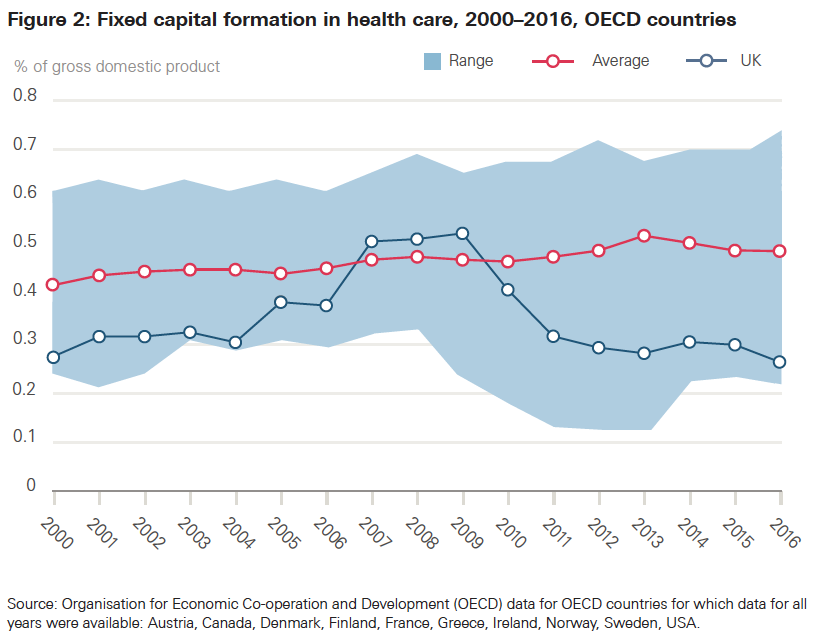
And said:
"Capital spending is a critical input in health care, with new technology able to transform services and improve workforce productivity.
The DHSC has proposed a more technology–and data–driven NHS. New technology and IT could improve patient services and increase productivity, but both currently make up a small proportion of capital spending."
So, not only does the NHS get starved of capital spending in general but the mix is very light on the things that would typically have the biggest impact on productivity.
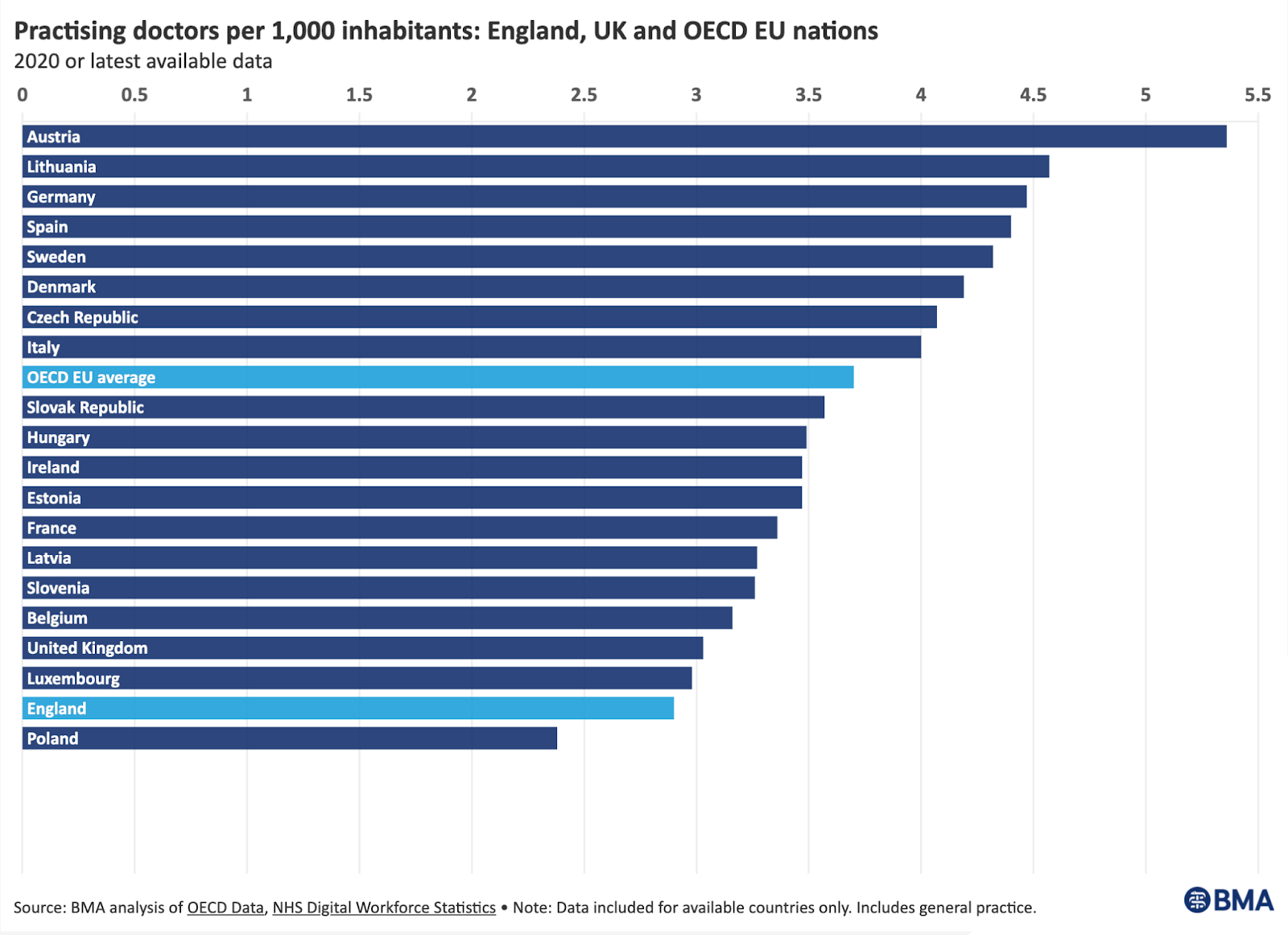
The result of this is that the capital employed per worker (an interesting measure of the stock of things that partly determine productivity) is half that of most comparable systems.
And, according to the National Audit Office, even when the NHS gets allocated a capital budget, it frequently either underspends it or pilfers it in year to cover operating deficits. This is a perfect illustration of the political choice to take an easy path rather than the right one. And one that has, in effect, killed the hope that NHS productivity could improve enough to lower the financial burden on long term government spending. And this has been the chosen path for two decades. It is little wonder that the productivity of the NHS is falling and that the system is creaking under the strain.
Some conservative commentators are now arguing that the government can no longer afford to keep spending more, as they need to do to stop the wheels from coming off the bus. But those commentators ignore a major reason for the current need for more spending: the neglect of any attempt to spend the money on the long term things that would make the NHS much more productive and reduce the pressure to spend more to avoid imminent catastrophe.
And the opposition don't help pull the debate back to solid ground by claiming everything is about staff shortages. There are two problems with this. One is that investment in better equipment and facilities could improve productivity so much the need for more staff could be reduced. The other is that the biggest reason staffing is a problem is not recruitment, it is retention and a large part of that is caused by the poor working environment some of which is caused by the lack of capital per worker. And the constant churn of staff, especially when experienced staff are replaced by cheaper but less capable staff, undermines team productivity and quality, exacerbating the need for yet more staff in some sort of anti-productivity death spiral.
So what?
And this brings us back to why the NHS is a microcosm of the economy as a whole. In order to attempt a rescue of government finances ravaged by the Kwarteng mini-budget, the key proposals to recover the government deficit currently being discussed are to cut things that are easy to cut quickly. Like capital spending. So, instead of spending on the long term things that enhance future productivity, they are likely to cut them further and in ways that damage the very growth they seek. They should have learned from the Osbourne era that that does not work. The easy path then–capital austerity–hurt the national growth rate and made it harder to fund the sorts of spending the government cannot cut if they don't want to lose their core voters (are they going to cut pensions when the most conservative block of voters are pensioners? I don't think so).
As Martin Wolf said in a recent column in the FT (my highlights):
The UK’s longer-term economic performance must indeed improve if the desires of its people for a better life are to be realised. If the government wants to do something useful about this, it might dust off the report of the London School of Economics’ Growth Commission of 2017. Better incentives are indeed a part of the answer, but only a part. This is why systematic tax reform would be desirable. There must also be difficult deregulation, notably of land use. The state must supply first-class public goods, in the understanding that these are a social benefit, not a cost. There must be fiscal and monetary stability. There must be far higher investment in physical and human capital, both public and private.
Neither the economy nor the NHS will be better tomorrow if the investment in the long term is cut. The persistent habit of picking easy cuts rather than the right cuts is a recipe for long term catastrophe (and possibly short term catastrophe too).
Spending the money well (especially not neglecting long term investment) is the solution to the growth and productivity problem in the NHS and the wider economy. Spending it badly by making easy choices now is not.
PS that cartoon is modified from an original by the late great B Kliban. See some of his other quirky cartoons here: https://www.gocomics.com/kliban