Our GPs are probably grossly overworked. There is plenty of evidence that this is true, but recent data collected by NHS Digital paints an ambiguous picture. Many GPs have reacted to my analysis of that data with incredulity, claiming NHS Digital don't know what they are doing. Or that the data is meaningless and too much of a burden to collect. The real situation is more complex and won't be fixed by NHS Digital alone but requires GPs to pay more attention to how they collect data and why it is collected. And it is critically important that the system does a better job of collecting data about their activity or the case for higher primary care funding will fail as soon as it is examined by the treasury. GPs, their system providers and NHS Digital all need to work together to create more useful data.
Recently released data poses some interesting questions for GPs
At the start of 2019, NHS Digital released the first public version of a new dataset on GP activity they had been collecting since the end of 2017 (and they are currently updating monthly). This dataset summarizes the number of consultations each day using data collected directly from the (major) providers of GP clinical systems (not all of the minor providers are covered yet).
The public version of the dataset covers the CCG-level aggregate number of appointments and the status of those appointments in several different categories:
- The appointment mode (face to face, telephone, visit, video etc.)
- The appointment status (basically whether the patient turned up for a booked slot or not)
- The type of staff who saw the patient (essentially whether the person who saw the patient was a GP or someone else)
- The delay between the booking and when the appointment actually happened
The data coverage is good for most CCGs (only one has no data at all) and there are some big, interesting insights in the data. For example, the number of no-shows ("did not attend" or DNAs) is very strongly related to the length of time a patient has to wait for an appointment (see my analysis here and a discussion in the BMJ here including comments on why the results are different to some previous academic analyses of DNA causes).
But the analysis I did on the number of appointments per day done by GPs caused a much bigger kerfuffle. I want to be fair and present those criticisms alongside the analysis. It is possible that both the analysis and GPs criticisms of it are right, but, if that is correct, then GPs, their systems providers and NHS Digital need to make some significant changes to how they work.
Before we start, a thought experiment
To put the results in context, it is worth doing a simple thought experiment to put the results in perspective.
Imagine a GP who does nothing other than see patients. She fills her entire 8-hour working day with 10-minute appointments with no breaks. Let's also assume that she works 48 weeks out of 52 (including bank holidays in the 4 weeks of downtime). And let's assume that each day worked consists of 48 appointments (this is how many fit into an 8-hour day if she takes no breaks between appointments or for lunch and does any other work after hours or at weekends). That means she does 11,520 appointments per year or about 44 per weekday in the year (she doesn't work every weekday because of holidays).
That 44 appointments per day doesn't sound like a sustainable workload. So let's assume a 1hr lunch break and gaps between appointments that brings the average work done down to 5 appointments per hour. Now she does 8,400 appointments per year or about 32 per weekday averaged over the year. That's probably still not sustainable every year but it is a thought experiment and we can make the simplifying assumption that GPs are superhuman. Bear this number in mind when we look at the actual reported workload from the NHS Digital data.
And, don't forget, that a real GP also has a ton of paperwork to process plus they need time for professional development, time to train new GPs and other staff and time to manage the practice. So lots of other work to fit into the actual working day alongside the 8-hr shift spent actually doing appointments. And, remember this analysis simply takes the total number of appointments recorded in a CCG divided by the number of weekdays and the number of FTE GPs; it ignores all the other work and all the extra time GPs put in beyond normal hours or at weekends.
What does the NHS Digital data show?
The original claim that prompted me to look more closely at the NHS Digital data was a simple calculation about the number of appointments per GP based on the headline numbers. NHS Digital estimate that about 307m appointments were recorded in the year to April (they adjust the total for missing data and their adjustment seems to differ from mine by about 10m/year but this is not a huge gap given other uncertainties in the data). Taking their number per working day in the year and adding the March estimate that there are 33,425 FTE GPs in England suggests that the average GP does about 35 appointments per working day. This seems to confirm, when compared to my thought experiment above, that the typical workload is well into unsustainable territory with a side order of "if we keep this up we are all going to die of overwork".
But that isn't what the dataset actually says. GPs have a lot of other staff who handle >40% of the patient contacts according to the data (this is the national average but see the map below for the variation among different CCGs in the % seen by non-GPs).
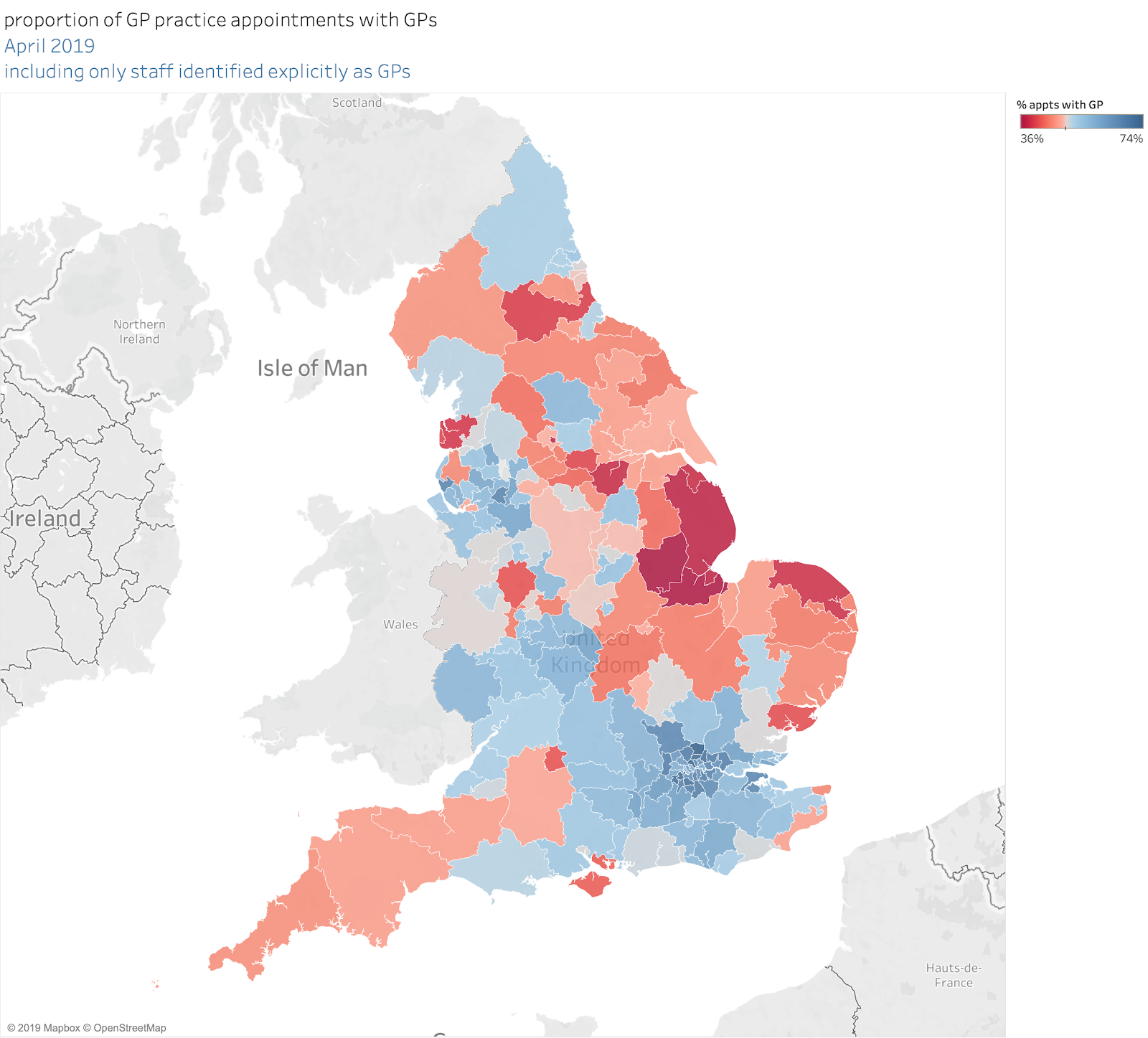
If you take that into account, the data actually says the average GP does something closer to 20 appointments per day.
20 appointments/day is the England average. But, usefully, we have the staff census data that tells us how many FTE GPs there are in each CCG and the appointment counts are available for each CCG as well. So I can do a CCG-level analysis and look at the variation across the country (taking into account the number of GPs in the CCG and the % of appointments with a GP). If we generously assume that activity where the staff type for the staff fulfilling the appointment is "unknown" is done by GPs we get the following distribution:
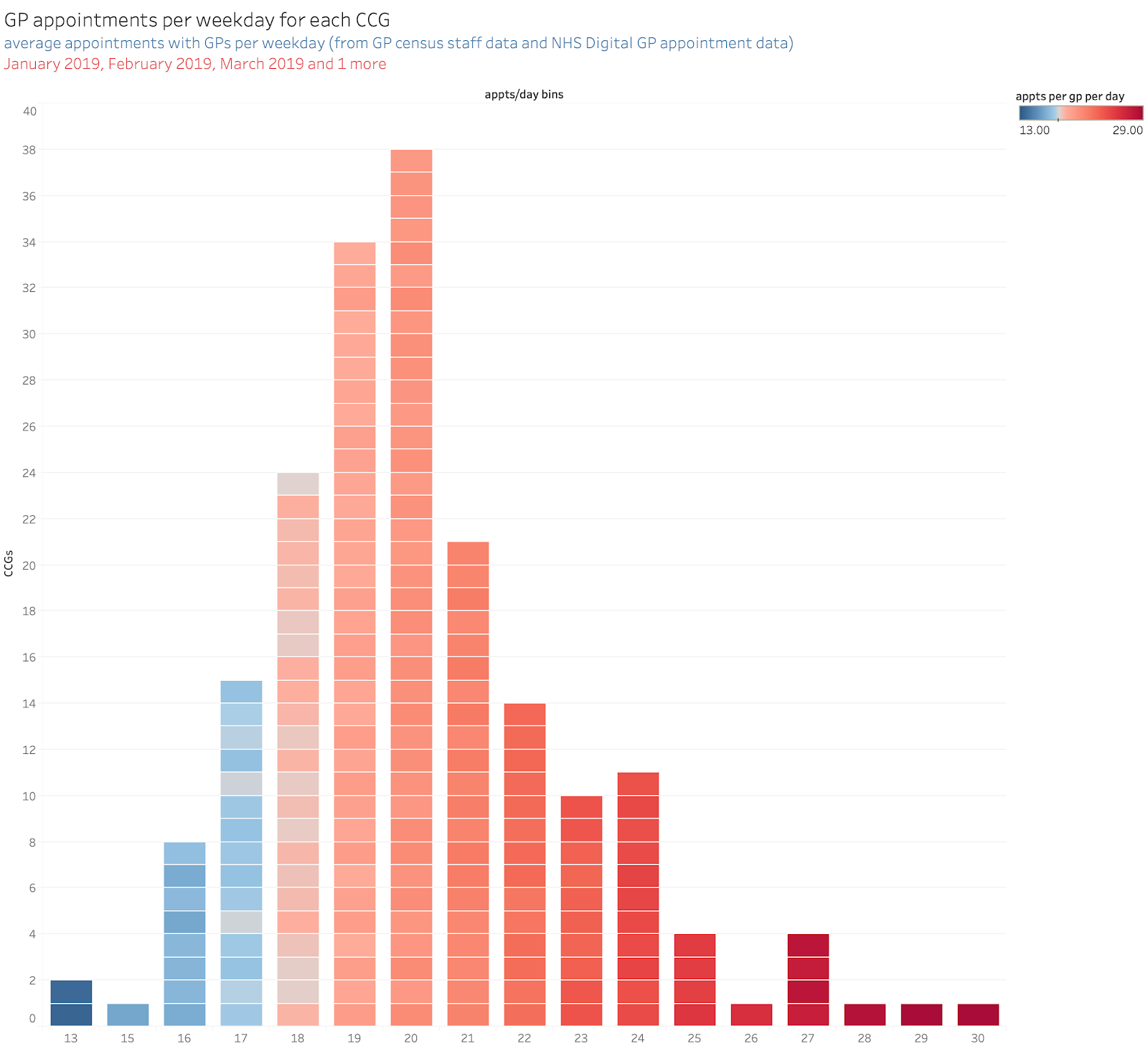
(Note: each block on this chart is a single CCG and the activity data is based on activity done on weekdays in the first 4 months of 2019. Also note that an interactive version of the dataset and many analyses is available here and you can test how varying some of my assumptions changes the results.)
In about 8 CCGs the GPs appear to be seeing an average of about 26-30 patients per day. The commonest CCG average is, however, closer to 20/day. Also, don't forget, the results are averaged over at least a month and reflect the average activity on all available days, not just the busy days where all the GP time is devoted to seeing patients.
Don't forget, though, that this is the average across a whole CCG: the variation among practices within each CCG is probably large so there will probably be some practices where the GPs do >30/day even when the CCG average is just 20.
Some GPs were indignant when I put an early version of this chart on Twitter. The typical response was "20 a day! I do far more work than that in a typical day. NHS Digital don't know what they are doing. The data is obviously rubbish…". I'm not entirely convinced that all the criticisms are fair, but it is worth looking at some of them to see if there are lessons to be learned.
Possible problems with the data
This just doesn't reflect my typical day
This could be because the data is just wrong, but we will come to that possibility later.
Another possible explanation is that what GPs remember about how busy they are isn't an accurate reflection of the average number of appointments across the whole month or year. If, for example, what GPs remember are the day when they are focussed on seeing patients but they also devote other days to practice management, paperwork, training or some other work that doesn't involve booked appointments, then their memory won't match the averages reported here: the results will reflect the total appointments divided by the total available time for all work not just the typical day when the GP is dedicated to seeing patients.
This work (and my initial thought experiment) assumes a 40hr week. Many GPs spend a lot more than 8hrs a day working (perhaps doing all the admin in their unpaid overtime). This dataset is not recording that work or adjusting the available hours to account for it. This doesn't impact the results but it may make the perception of the results much less clear than they should be.
The data clearly is missing a lot of the work we do
Part of this is a perception problem as discussed above. But it could clearly be true that a lot of activity is not correctly recorded.
But the blame here isn't on NHS Digital. The data is directly collected from the major clinical systems used in practices to record activity. If the numbers are a big understatement of the appointments being booked, then practices have a big problem not just NHS Digital. I suspect we are not understating the true number of appointments by a large margin.
But we could be understanding the amount of activity. Many patient contacts don't result in a booked face-to-face appointment. GPs do some work online or by telephone. Clinical systems are not uniformly good at recording that activity as I know from comparing incoming requests via askmyGP (an online tool that manages all incoming patient requests and helps GPs to completely change their workflow when responding to those requests in ways that improve the speed of responses to patients and lowers the degree of overwork for GPs). Successful online tools (and some phone-triage approaches) often result in only 1 in 3 requests leading to a face-to-face appointment. This reduces the number of appointments recorded in the clinical system while providing satisfactory responses to the other patients. But much of the activity for those other responses may never appear in the clinical systems. As GPs adopt new ways of working their clinical systems may become a lot less good at measuring their activity.
On the other hand, the NHS Digital data does record a lot of phone activity. Between 10 and 15% of all appointments are recorded as taking place online, by phone or by video. We know that recording of this is patchy, but so is uptake of alternative ways of responding to patient demand. Some GPs still think that face-to-face appointments are the only response despite mounting evidence that offering a wider range of alternatives can reduce GP workload and make patients happier because they get a faster response.
We have to admit, though, that traditional GP systems have not caught up with this change in practice and won't consistently record the shift in activity reliably.
NHS Digital will draw all the wrong conclusions from these results
I got the impression from some comments on my initial analysis that, not too exaggerate too much, central NHS bodies are just a bunch of malingering bureaucrats who exist just to malign hard working GPs by misrepresenting how hard they work by providing the NHS leadership with false, irrelevant data about what they do. And that any suggestion that this should be fixed by GPs spending more time to provide accurate data about what they do would be yet another straw added to the already broken camel's back that is the typical GPs unsustainable workload (or some such mixed metaphor for even more overwork).
But NHS Digital's motivation is not to burden GPs with more work or to undermine the case for more GPs. It is to understand what GPs are doing to develop better policy, and that can't be done without better data. Originally the idea was focussed on developing a better understanding of winter pressures but it should be useful for bolstering the case for more investment in primary care or for promoting better working processes.
But, imagine the conversation the NHS would have with the treasury when bidding for the money to recruit another 5,000 GPs:
NHS "We need another 5,000 GPs."
HMRC "How much will that cost?"
NHS "A couple of billion pounds a year."
HMRC "That sounds like a lot. Why do you need it?"
NHS "They keep telling us they are overworked."
HMRC "That's what everyone says. How much work do they do? Show me some numbers."
NHS "They say they are doing unsustainable numbers of appointments a day."
HMRC "How many is that."
NHS "We don't know exactly but more than 30/day doesn't sound sustainable"
HMRC "So how many are they actually doing?"
NHS "No idea. But I'm sure it is a lot. We really need the money to recruit more GPs."
HMRC "Sure. You can have it when we cash the £350m/week we will save from Brexit."
NHS "Really?"
HMRC "No."
HMRC "We were joking. Sod off and don't come back until you have some actual evidence."
OK, I'm parodying the case for more money for GPs and there are other hard sources of evidence that say they are overworked. But if the NHS as a whole doesn't understand what, in detail, GPs are actually doing any case for reform or extra cash is going to look weak.
There are more reasons than this to have reliable data. GPs need it to understand their own work or they won't have any idea how to do a better job. While the NHS Digital appointment data doesn't capture everything they do, it is at least a start providing a better understanding of a large part of their activity. And the main limitations that prevent the data being more useful are not NHS Digital's fault but the fault of the system providers and choices made by GP practices.
The data isn't consistent or comprehensive
GP Clinical systems are built around a model of GP work that assumes everything revolves around a pre-booked face-to-face appointment. GPs can vary how they label the slots for activity in the system and they don't always assume every appointment is 10mins long (though their royal college doesn't seem to have caught up with this realisation). Systems usually allow the exact time taken for each appointment to be recorded (assuming GPs press the right buttons which they don't always do). Some systems make it easy to record activity in open-access clinics. But systems tend to assume every appointment slot is the same length and some are completely, irretrievably hopeless at measuring the time taken for consultations done by phone.
One of the biggest problems faced by NHS Digital is the number of different descriptions given as labels for each slot. Practices are, essentially, free to label each slot however they want and one estimate says that there are tens of thousands of different labels in use across practices in England. So when NHS Digital try to acquire data from everyone it is a gargantuan task to correctly identify the different types of appointment and group them together in ways that make sense. Was that a face to face pre-booked appointment? Or an ad-hoc on the day f-to-f as part of a walk-in clinic. Or a slot where a nurse did flu-jabs?
And, as more activity is initiated online and GPs choose to triage patient requests before booking appointments, there are more varied ways for GPs to respond to patients. And the systems–designed as they are around the idea that most activity involves pre-booked slots–don't record all those interactions. In practices using online tools like askmyGP only around ⅓ of requests result in a face-to-face appointment (e-Consult, another online tool provider estimates a similar ratio). This means, potentially, that the majority of GP activity won't be recorded in the traditional clinical systems.
So it may well be true that what NHS Digital are collecting is not a reliable guide to what activity GPs are doing. But the fault can't be fixed by them: if we want better data the problem has to be addressed by the practices (who need more consistency is how they use their systems) and the suppliers (who need to design their systems to break the model that everything neatly fits into 10 or 15min slots).
Some suggestions about how to do a better job
It is not at all helpful to complain that the NHS Digital GP data is rubbish. If we want to do a better job in primary care (to improve how GPs work and make an unanswerable case for more investment) we need better data.
When the four practices serving St Austell merged in 2015, it was an opportunity to reconsider how they did things. The GPs kept a diary, noting precisely what they got up to during the day. It turned out that lots could be done by others: administrators could take care of some communication with hospitals, physios could see people with bad backs and psychiatric nurses those with anxiety. So now they do. Only patients with the most complicated or urgent problems make it to a doctor.
The key point here is that only when they had reliable data about their activity could the GPs redesign the work they did in ways that would improve it.
In hospitals, routine datasets such as Hospital Episode Statistics (HES) give us insight into who gets treated, for what, by whom, and where. This basic knowledge of the activities and performance of hospitals is now essential for making evidence-based policy changes, monitoring existing policies and providing fundamental administrative data to run the system and allocate funds. There is a clear need for something similar in general practice…
But, they continue:
NHS Digital makes it clear that what has been released so far still needs improvement. As it stands, there are a number of problems with the data and these limit the extent to which we can use it as a resource for evidence-based policy.
Having different practice IT systems gives GPs flexibility over the way they organise their work. But the absence of reporting standards in general practice means information is recorded differently in each system, making it difficult to combine the data, and information gets lost.
In the early 2000s, hospital activity data (HES) was in a similar state of disorder. Doctors took little interest in making sure that the amount of activity recorded was correct or the clinical details correctly coded. They too argued that this was just an unnecessary bureaucratic task required puerly for "feeding the machine" (even though the most basic metric of hospital success–not killing your patients too often–requires accurate coding).
But HES got a lot better. One way it got better was to show medics what HES said about the work they did. The Royal College of Physicians ran some interesting experiments starting in 2002 (reported here and here). They took HES data and fed it back it to the clinicians whose activity it recorded. In one of the reports on this exercise they argue this:
A vicious circle ensues: routinely collected data is perceived as being of poor quality and unable to support the needs of the individual. Individual clinicians avoid the use of such readily available information... Centrally held datasets remain unchanged through neglect, clinicians failing to engage with the information process in their trusts and remaining ill at ease with the records of activity which result. It is clear that if this cycle is to be broken, steps must be taken to engage clinicians at a level whereby the information is made readily available, accessible in format and of use to clinical practice. By examining routine data from a clinical perspective and feeding issues of quality back to trust information departments the cycle can be reversed.
Hospital clinicians being shown their own data in a digestible form was a big part of the drive that improved the quality and utility of HES data. GPs and NHS Digital need to do something similar.
Perhaps NHS Digital could take the first step by making practice level data from the central collection available to practices in a useful, comprehensible format so GPs can see what the data actually thinks they did. This would be the first step in driving improvement in what is recorded.
Conclusion
In short, here are some simple ways for the different players in primary care to change what they do in ways that would promote real improvement for GPs and their patients.
NHS Digital should make a friendly, easy to comprehend, version of their dataset available to every individual practice so GPs can compare what they think they did to what NHS Digital's extract has recorded.
GP System Providers should make their systems more flexible in recording non-appointment activity and should work to support GPs to use more consistency in how they record and label their activity.
GPs and practices should not just dismiss the data as being unreliable and useless. They should strive to understand it and seek ways to work with NHS Digital to make the data useful for local purposes and more reliable for policy making.
Everyone should not dismiss data they don't like but engage with it and seek to make it both more reliable and more useful.
Thanks a lot for sharing a highly effetive content!
ReplyDeleteFind peace of mind with Spy World's GPS tracker for car. Keep tabs on your vehicle's location at all times. Trust Spy World for top-notch tracking technology. For any query: Call us at 8800809593 | 8585977908.