The NHS has plenty of problems to solve but it often tries to short-circuit effective solutions by not bothering to check whether the problem has been correctly understood or the solution is likely to work. The system's pathological hostility to data makes this worse. As a result the NHS devotes a great deal of effort into futile actions which demoralise staff because they don't work.
I first started working for the NHS in 2002 when the 4hr A&E target was originally set. I helped compile the national performance reports to monitor progress and I designed some of the first analyses that used patient-level data to support improvement in individual departments. I learned a lot about the problem and what solutions were effective.
In those bad old days treatment was often unbearably slow and sometimes unsafe. There were plenty if ideas about why A&E was so often slow and even more ideas about how to speed the typical A&E journey up. Most of them were wrong. I could tell that because I looked at the data.
Some people thought that the target was a bad idea. It grated with the belief in many doctors that the sickest should get the fastest treatment. Many thought it was impossible. But it proved to be very possible and it also proved to be good for patients. Recent evidence has confirmed that long waits kill: speedy A&Es are not just a patient-pleasing idea, they actually save lives.
Nearly a decade and a half later discussions about the latest A&E performance crisis (we are not yet quite as bad as we were before the target was set, but progress towards that ignoble goal is rapid) are still mired in many of the ideas that were shown to be wrong when I collected the first data. Political debate, medical discussions and improvement plans are still full of zombie ideas that some of us already know won't work.
It isn't just A&E. Zombie ideas are more or less an SOP in many strategic plans across the whole NHS.
This is maddeningly frustrating for those of us who are used to applying evidence to improving the system. Why is so much effort going into ideas that won't help?
I've got a theory: the NHS doesn't know how to solve problems. Instead of doing the hard work of diagnosis and testing, it leaps to implement solutions purely on the basis of their superficial attractiveness. It seeks magic bullets. It focusses on symptoms not causes. It fails, repeatedly.
The diagram below sums up part of the problem. It is based on some thinking from one of the few good books on business strategy (which is, after all, a problem solving process): The Mind of the Strategist.
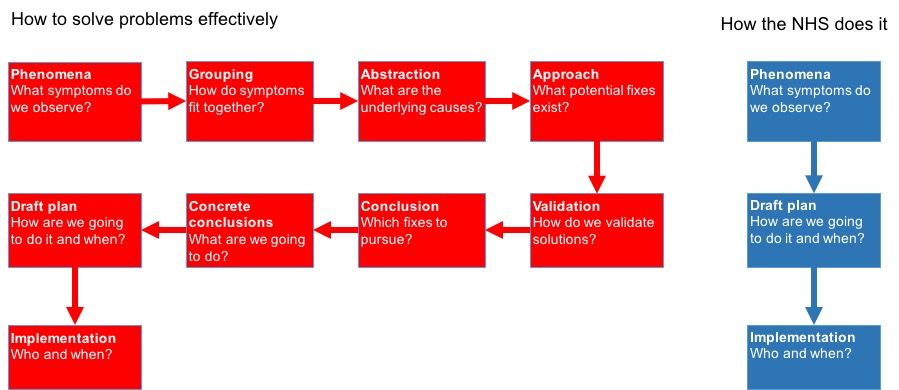
It's author starts from the position of trying to understand why so many business strategies fail and the diagram summarises some of his thinking. The ideas are generic to any type of problem solving which is why they apply so well the the NHS.
Here is my take. The NHS is like a doctor who doesn't want to take the time to really understand what is wrong with her patient and offers palliatives to the superficial symptoms without seeking the underlying causes. Sometimes a headache is just a headache and an aspirin will cure it; other times it is meningitis or a brain tumour and a failure to diagnose correctly kills the patient. Few problems in the current NHS can be cured by the organisational equivalent of an aspirin.
My theory of what is broken explains many strategic and operational failures in the NHS and is the best explanation for why they system as a whole seems to find improvement so hard to sustain.
Dysfunctional thinking leads to poor solutions to problems
My specialist topic is A&E performance and improvement. So I see a lot of misconceptions that frustrate me. Here are some examples.
So people observe that performance is poor. They notice that their A&Es are busy. They leap to the conclusion that they are being overwhelmed by demand. So they propose solutions that are based on diverting patients away from major A&Es.
Or, they note that staff appear overworked and the department is crowded. So they leap to the conclusion that the problem is A&E understaffing (and, perhaps depending on how political they are, they blame this on government underfunding and a national shortage of A&E staff).
But these supposed diagnoses ignore other important observations. There is no relationship at all between A&E attendance and performance either nationally or in individual departments. Mostly, for example, attendance is higher in the summer but performance is worse in the winter. Some of the worst performing departments right now are places where attendance has been steady for several years.
It isn't a staffing problem either. We might have fewer staff than many departments (or the RCEM) would like but we have a lot more than we had 5 years ago (when performance was much better). In fact there are about 50% more A&E consultants than there were 5 years ago and total staffing has grown faster than attendance for some years while performance has continued to decline.
I won't quote the details of this analysis here, but it has been studied a lot. Those studies have had very little influence on the system's choices about strategy or the general discussion on the topic.
The single biggest problem causing poor A&E performance is not even inside the A&E: it is the problem of accessing beds in the hospital. This has been obvious since I first started collecting data about A&E problems. The disease is poor flow through beds. If the treatment is adding more staff in A&E you are merely dealing with the symptom and failing to address the cause of the underlying problem. It's a bit like treating a blocked toilet with some anti-constipation medicine: it's irrelevant and probably makes the problem worse.
Somehow the system keeps coming up with solutions by leaping to conclusions about the symptom and forgetting to do the hard work of identifying the underlying disease. This is exacerbated by a habit of looking only locally and not at the whole system (in a hospital each department looks for its own internal problems but forgets it is part of a system where local initiatives may affect other units and other units may be the cause of its problems).
Big system-wide initiatives seem to suffer from the same problem. When hospital costs are too high the idea of mergers often arises. This seems to be driven by the belief that economies of scale are a major driver so bigger should be cheaper.
There are two problems with this. One is that it doesn't seem to work (few mergers seem to have delivered notable cost savings and many have made things worse). The other is that economies of scale may be all that some economists can imagine, but they seem to only account for about 10% of the differences among hospital costs. But that second observation requires a great deal of analysis and number crunching which isn't much of a part of NHS strategizing.
One thread running through many improvement initiatives is the need to be seen to do something. The NHS would do better to stop doing something until the correct problem has been identified or there will be no energy or resources left to do the right thing.
So what?
The NHS needs to stop leaping to the first solution it thinks of. If the system is to stop wasting the investment it makes in improvement it needs to stop and think.
Look at the whole system not just the local system (so don't assume that problems in A&E, for example, are caused purely in A&E) and group the different symptoms together. And look at the data. We have known since we started collecting data about A&E performance that the overall volume of attendance is not the problem and has no relationship with speed of treatment, but both locally and nationally solutions are still being proposed that involve diverting patients away from A&E.
When you have a picture of how the whole system is performing, develop and test some ideas about what the underlying problem is. For example, many different hospital problems seem from my analysis to be caused by system flow through beds. This idea explains both poor A&E performance and poor ability to reduce elective waiting lists.
What solutions exist? How about actively managing flow across the system? Most hospitals don't even collect the data necessarily to understand how flow works or what actions can make it better. Instead of seeking that data and the understanding and insight that would come with it, most seem to rely on local tinkering (more staff in A&E, extra clinics at the weekend to clear the waiting list backlog). These won't address the underlying blockages in flow through the beds. Worse, some don't try to fix anything relying on assigning blame for the problems on uncontrollable outside factors (which is why there is so much discussion about delayed transfers of care which are a big problem cause by social care, but not the biggest problem as more discharge delays are inside hospital control).
Fixing flow isn't easy, but it is a lot harder if you don't even admit that it is the key problem. Practical solutions (like having the data to know where all patients are all the time) are hard to implement. But doing easy things that don't work is worse than having to experiment with hard things that do. Because repeated failed initiatives sap the energy of staff and waste resources, making doing something different in the future even harder.
The same general observations apply to other problems. The NHS as a whole has to learn that doing the wrong thing because you haven't spent the effort to identify the right problem and the right solution is worse than doing nothing at all.
No comments:
Post a Comment