A shortage of A&E staff isn't the reason for poor performance in A&E. It never has been. Some A&Es have shortages of staff and that is a problem, but is clearly isn't the result of a national shortage of qualified staff. And the more the RCEM lobby for more staff the more they detract from accurate analysis of the real problems of A&E. Fix those and we might even fix the local staff shortages.
If you read the newspaper headlines or the press statements issued by the Royal College of Emergency Medicine (RCEM), you might believe that we are desperately short of qualified staff in A&E and that is the reason performance is current at dismal record-breaking lows. You would be wrong.
You might also believe that the reason why some A&E departments struggle to maintain safe levels of medical staffing is because there is a declining number of A&E doctors or because we are desperately short of A&E doctors. But this certainly isn't the cause of local shortages and whether we are short of the ideal number of A&E medics is certainly not the reason why performance is poor.
You might, in responding to one of my many complaints that misleading things are being said about A&E staffing which is growing faster than any other specialty, argue that attendance has outpaced growth. You would still be wrong.
Don't get me wrong, an understaffed A&E department is not good and is not safe. And there are several departments in England where staffing is far too low (they are the ones generating all the ink in headlines giving the RCEM an excuse to lobby for more doctors). But blaming those local shortages on a national shortage is misleading and distracts attention from the real problems. And blaming local shortages on "NHS cuts" or squeezed budgets is ludicrous.
For a start, the local departments who are severely understaffed have the budget for more A&E staff but they can't recruit them. That's a recruitment problem not a budget problem. You could plausibly argue that those local problems were the result of a national shortage. That's a reasonable argument but falls down because the majority of A&E departments don't have problems recruiting. People being unwilling to work for your department might be caused by purely local problems like the fact that the department is badly managed and is a really bad place to work. Arguing about the national numbers of doctors isn't going to fix that. And lobbying for more staff actively detracts from identifying the local issues that need to be fixed to actually address the problem.
And the national numbers don't show the things headline writers assume they show. Here is a chart (based on ESR data) showing the national number of doctors with an A&E specialty:
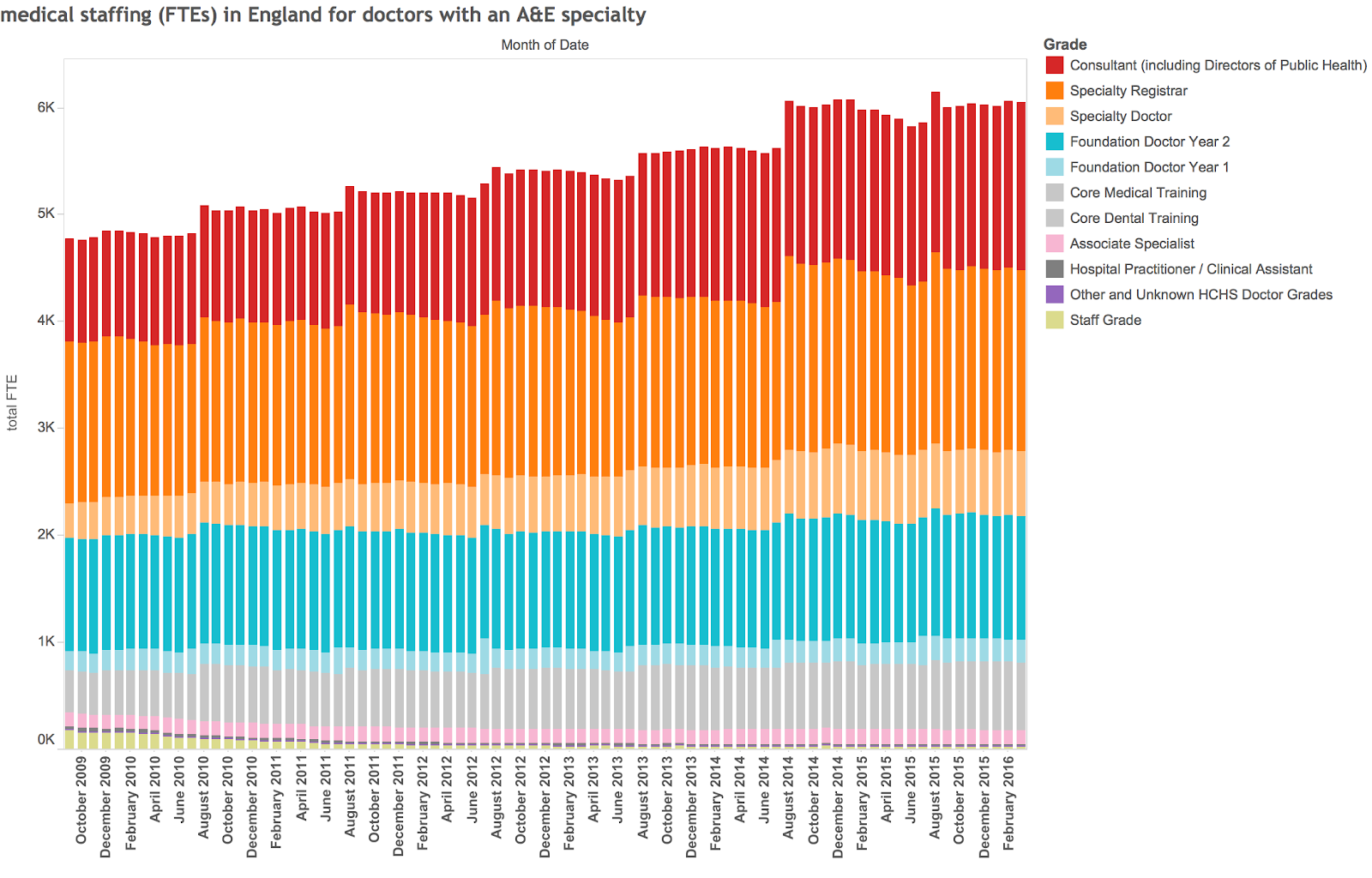
Total medical staff in A&E have increased by more than 20% over this period; consultant levels have risen by more than 50%. Over this time attendance at major A&Es has risen by about 12% (so staff are not being "overwhelmed by demand" as the common belief has it).
So we have more A&E doctors but do we have enough? The RCEM have a model that says we still don't. And their model might be right, but we are clearly closer to their recommended level of staffing that we have ever been so hinting that current problems in A&E are caused by an increasing shortage is just bollocks. We can have a rational debate about the right number of A&E doctors nationally but that debate has nothing to do with the local problems in some A&Es or the current performance of the system.
So why do perceptions differ so much?
One of the biggest reasons is a failure of many to grasp the distinction between demand and queues. In A&E the flow of patients into the department isn't the primary cause of the department being busy: that would be caused by the number of people waiting. But the queue of people waiting is a lot more sensitive to the speed of the flow than it is to the number turning up. When the flow slows down, the queue expands quickly and that is what the staff perceive as the workload. But they mistake this for an issue with demand or attendance (we know this isn't true as the we count the attendance numbers and they have not suddenly increased.)
There is a good reason why flow in A&E has got slower and it also explains why A&E staffing is irrelevant to the speed. Flow is slow because we can't find empty beds for patients who need to be admitted (go read some of my other analysis of this especially the one where I point out the key problem is beds). Even doubling the staff number in A&E would not make any more free beds appear in the hospital.
More significantly, the performance problems caused by poor flow through beds may go a long way to explaining why some departments struggle to find enough staff. The direction of causality is not poor staffing -> poor performance it is poor performance -> poor staffing. I've observed departments which are very crowded because of problems getting patients into beds. The A&E medics still try improvement initiatives but they don't make much difference. They can't as they don't address the bottleneck in the flow which is outside the A&E. This increases frustration and adds to the depressing environment of being in a crowded department where nothing you do makes things better. Eventually people don't want to work there any more. Hence: recruitment crisis and staff shortages. But the correct answer isn't more A&E staff: it is to address the bottlenecks in flow which are mostly outside the A&E. Improving flow makes the A&E less crowded and makes the work there less stressful.
Lobbying for more A&E doctors to fix this sort of problem is irrelevant, ineffective and a serious distraction from dealing with the real problem. That's why I object so much when the RCEM use local problems to lobby for more A&E doctors nationally.
And talking about a mythical national shortage detracts from other analysis the RCEM does, most of which is good and almost all of which is more important than the national number of A&E doctors.
Some truth in what you're saying. Exit block is the biggest issue we face as ED docs. It causes awful pressure on our staff and is dangerous. You have failed to mention the steep decline in the performance of ED juniors. Seeing 20 patients in a 9 hour shift was the norm 15 years ago, now we are lucky to get half that even when the phlebs do all the lines and bloods and the RAT doc orders the x-rays. THAT is a key factor when looking at workforce planning. Junior doctors, for a variety of reasons, cannot see patients at an acceptable rate
ReplyDelete